Visual migraine refers to temporary visual disturbances caused by migraine: most commonly the classic aura of zigzag lines (fortification spectra), blind spots (scotoma), or shimmering patterns that spread across the visual field over 20 to 30 minutes. These symptoms originate in the visual cortex of the brain and affect both eyes simultaneously. They are usually followed by headache but can occur without any headache at all. Visual migraine is distinct from ocular migraine, which originates in the eye itself and typically affects only one eye.
The first time it happens, visual migraine is terrifying. A strange shimmer appears near the center of your vision, and within minutes it grows into a curved arc of flickering zigzag lines that slowly expands until it passes out of your visual field. Many people are convinced in those moments that they are having a stroke, going blind, or experiencing a brain event. If this has happened to you, you are not alone, and what you experienced was almost certainly a migraine aura: frightening, but typically benign and fully reversible.
Understanding what these visual symptoms are, why they happen, and when they genuinely warrant concern can transform something frightening into something you can navigate.
What Is Visual Migraine?
"Visual migraine" is a lay term that typically describes one of two related conditions:
1. Migraine with visual aura (most common) The classic scintillating scotoma: a crescent-shaped arc of flickering zigzag lines that usually begins near the center of vision and slowly expands outward over 20 to 30 minutes, leaving a temporary blind spot (scotoma) in its wake. Both eyes are affected because the disturbance originates in the visual cortex of the brain, not in the eyes themselves.
2. Ocular migraine (retinal migraine) Visual symptoms affecting only one eye, caused by transient reduced blood flow to the retina. True ocular migraine is much rarer. Covering each eye alternately distinguishes it from visual cortex aura. If the problem disappears when covering one eye, it is likely retinal (ocular). If it persists regardless of which eye is covered, it is cortical, meaning typical migraine aura.
When most people search for "visual migraine" or "optical migraine," they mean the first type: cortical visual aura. This article focuses primarily on that. For retinal migraine specifically, see the ocular migraine guide.
What Does Visual Migraine Look Like?
Scintillating Scotoma (Most Classic)
The hallmark visual migraine experience:
- Begins as a small flickering spot or arc near the center of vision
- Grows into a curved or horseshoe-shaped arc of shimmering, zigzag lines
- The pattern moves slowly outward toward the periphery over 20 to 30 minutes
- The outer edge is bright and scintillating (flashing, sparkling)
- Inside the arc is a blind spot: an area of lost or blurred vision
- Eventually passes out of the visual field toward the periphery
- Total duration: typically 20 to 30 minutes
- Vision returns completely once the arc passes
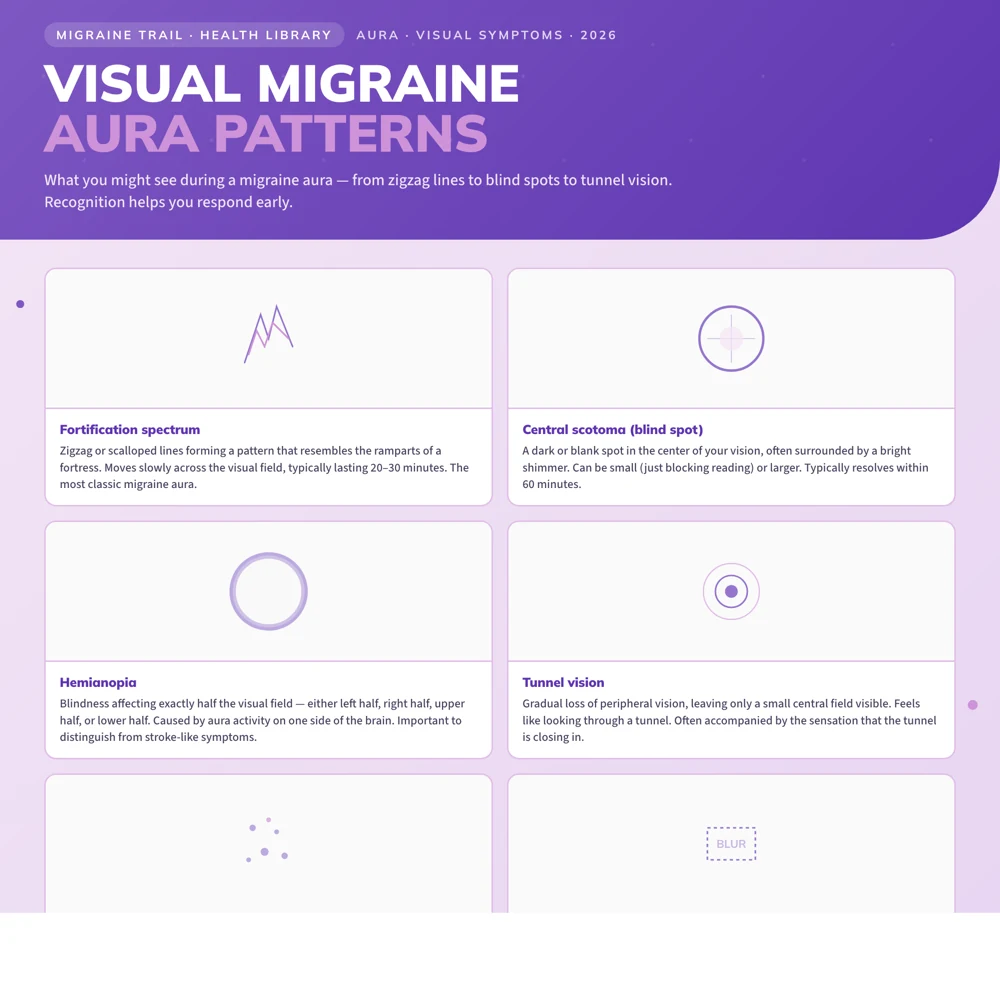
The zigzag edge is sometimes called a "fortification spectrum" because it resembles the star-shaped walls of medieval castles when viewed from above.
Visual Snow
Some people with migraine experience visual snow: a persistent or episodic visual phenomenon where the entire visual field appears to have fine static or flickering dots overlaid on it, similar to an old television tuned to a dead channel. Visual snow syndrome is increasingly recognized as a distinct condition closely linked to migraine with aura. Unlike a typical scintillating scotoma, it can persist between attacks.
Other Visual Aura Types
- Positive phenomena: Flashing lights, colored lights, sparkling dots, phosphenes (light flashes with eye movement)
- Negative phenomena: Blind spots, loss of a segment of the visual field, blurred patches
- Distortion: Objects appearing larger, smaller, or distorted
- Kaleidoscope vision: Fragmented, mosaic-like visual disturbance
Without Headache: Silent Visual Migraine
Visual aura occurring without any headache is called migraine aura without headache, or sometimes "acephalgic migraine" or "silent migraine." This is more common than most people realize. Up to 20 to 30% of migraine with aura episodes may occur without significant headache, particularly in older adults. A person can experience the full scintillating scotoma with no head pain at all, or only mild discomfort.
This can be particularly confusing if you have always associated migraine with severe headache. If you are experiencing visual disturbances without pain, they can still be migraine, and they still deserve medical attention if they are new or changing.
What Causes Visual Migraine?
The cause of visual aura is cortical spreading depression (CSD): a slow wave of electrical activation followed by suppression that sweeps across the visual cortex (occipital cortex) at approximately 3mm per minute.
This is the same speed at which the scintillating scotoma grows and expands across your visual field. The zigzag line you see is essentially the wavefront of the CSD wave passing across your visual cortex. Once this was understood, the visual experience stopped being mysterious. You are essentially seeing your own brain activity.
As CSD sweeps through cortical tissue, it:
- Initially activates neurons, producing the positive visual phenomena (flashing, sparkling, zigzag lines)
- Leaves temporary suppression in its wake, producing the scotoma (blind area)
- Activates the trigeminal nerve endings at the edge of the cortex, triggering the headache that follows
Visual Migraine vs. Ocular Migraine: Key Differences
| Feature | Visual Migraine (cortical aura) | Ocular Migraine (retinal) | |---|---|---| | Origin | Visual cortex (brain) | Retina (eye) | | Eyes affected | Both eyes simultaneously | One eye only | | Pattern | Expanding arc, zigzag lines, scotoma | Monocular loss, graying out, mosaic | | Duration | 20 to 30 minutes, gradual expansion | Usually under 60 minutes | | Headache | Often follows | Often follows | | Diagnosis test | Persists with either eye covered | Disappears when affected eye covered | | Stroke concern | Low (bilateral = cortical = benign) | Higher (monocular = vascular) |
The single-eye test: If you notice visual symptoms, cover one eye. If the symptoms are present regardless of which eye is covered, the disturbance is cortical, the benign, typical migraine aura. If covering one specific eye makes the symptoms disappear completely, the affected eye is the source, which warrants urgent evaluation.
Is Visual Migraine Dangerous?
For most people, typical visual migraine with classic scintillating scotoma is not dangerous. It represents neurological activity in the visual cortex, uncomfortable and alarming, but benign and fully reversible. Many people learn to live with it, to recognize it as a familiar (if unwelcome) signal, and to act quickly when it appears.
However, visual symptoms can occasionally represent something more serious. See a doctor or go to the ER for:
- First-ever episode: any first visual disturbance needs evaluation to rule out TIA, retinal detachment, or other causes
- Monocular symptoms (one eye only, especially if sudden or painless): could be TIA, retinal artery occlusion, or amaurosis fugax; seek urgent evaluation
- Sudden complete vision loss: always a medical emergency
- Symptoms lasting more than 60 minutes: prolonged aura needs assessment
- Symptoms accompanied by weakness, speech difficulty, or confusion: could indicate hemiplegic migraine or TIA
- Sudden onset "worst ever" symptoms, especially with severe headache
Please trust yourself on these. You know your body. If something feels different from your usual pattern, it is always right to get it checked.
Migraine With Aura and Stroke Risk
Migraine with aura is associated with a mildly elevated risk of ischemic stroke, approximately twice the general population rate. This risk is concentrated in:
- Women under 45 who smoke
- Women taking combined oral contraceptives (estrogen-containing): combined oral contraceptives are contraindicated in migraine with aura
- People with multiple cardiovascular risk factors
The absolute risk remains small, but the association is well-established and guides treatment decisions. Smoking cessation and avoiding combined hormonal contraceptives are the two most actionable steps for reducing this risk. Please discuss contraception options with your doctor if you have migraine with aura.
How Often Does Visual Migraine Occur?
Visual aura frequency varies widely. Some people have aura with every migraine attack; others experience it rarely or only at certain life stages. Aura can increase significantly during perimenopause, for example, even in people who have had infrequent aura for years.
Aura can also occur more frequently than headache. Some people have one or more aura episodes per week without significant headache, particularly when taking preventive medications that reduce headache but not always aura, or during hormonal transitions. This can feel strange and disorienting, especially if you have come to associate aura with an incoming headache that never arrives.
Treatment
Visual aura itself does not have a specific treatment; the 20 to 30-minute episode passes on its own. The treatment goal is managing what comes after, and making the most of the warning window aura provides.
During aura:
- Rest in a quiet, dim environment
- If headache routinely follows, this is the ideal time to take migraine medication. Treating during aura, before severe pain develops, produces significantly better outcomes.
- Gepants (ubrogepant, rimegepant) taken during the prodrome or early aura may prevent or reduce the headache phase in some people
For the headache that follows:
- NSAIDs (ibuprofen, naproxen) and combination analgesics (Excedrin Migraine) for mild-to-moderate attacks
- Triptans for moderate-to-severe attacks (safe to use during the aura phase, though typically given after aura resolves in practice)
Preventive therapy: If aura episodes are frequent or disabling, discuss preventive migraine therapy with your neurologist. Options include beta-blockers, tricyclics, topiramate, valproate, and CGRP monoclonal antibodies.
Recognizing Aura as a Warning
Many people who experience visual aura learn to use it as a valuable early warning system. The 20 to 30-minute window of aura is an opportunity to:
- Take medication early, when it is most effective
- Move to a quiet, dark environment
- Cancel commitments before the headache hits
- Begin hydrating and prepare for what is coming
This is not a small thing. For many people living with migraine, having that warning, even a frightening one, gives them agency in a condition that can otherwise feel completely out of their control.
Track your aura episodes alongside headache data with Migraine Trail, noting aura type, duration, and what followed. This record helps confirm the aura-headache relationship in your specific case and gives your neurologist the structured documentation needed to guide treatment.