Hemiplegic migraine is a rare subtype of migraine in which the aura includes fully reversible motor weakness or paralysis affecting one side of the body (hemiplegia or hemiparesis). It can also involve speech disturbance, sensory loss, visual symptoms, and altered consciousness. Hemiplegic migraine closely mimics stroke and TIA, so any first episode requires emergency evaluation. It occurs in a familial form (inherited, with gene mutations in CACNA1A, ATP1A2, or SCN1A) and a sporadic form (same presentation, no family history).
Waking up and finding that your arm won't move, or watching your speech become slurred without warning, is terrifying. If you have hemiplegic migraine, you have likely lived through moments that felt like the ground was collapsing beneath you, perhaps in an emergency room with doctors uncertain whether you were having a stroke. The fear and uncertainty that comes with this condition is real, and it deserves to be taken seriously.
The good news is that attacks are nearly always fully reversible, and with the right diagnosis and treatment plan, most people achieve significant reduction in episode frequency and severity. You are not alone in this, and there is a path forward.
What Is Hemiplegic Migraine?
Hemiplegic migraine is classified by the International Headache Society (IHS ICHD-3) as a distinct migraine subtype under "migraine with aura." The defining feature is motor weakness as part of the aura, not just sensory tingling or visual symptoms, but actual difficulty moving or controlling one side of the body.
It affects an estimated 0.01% of the population (around 1 in 10,000 people), though it is likely underdiagnosed given how often it is mistaken for stroke on first presentation.
Two forms:
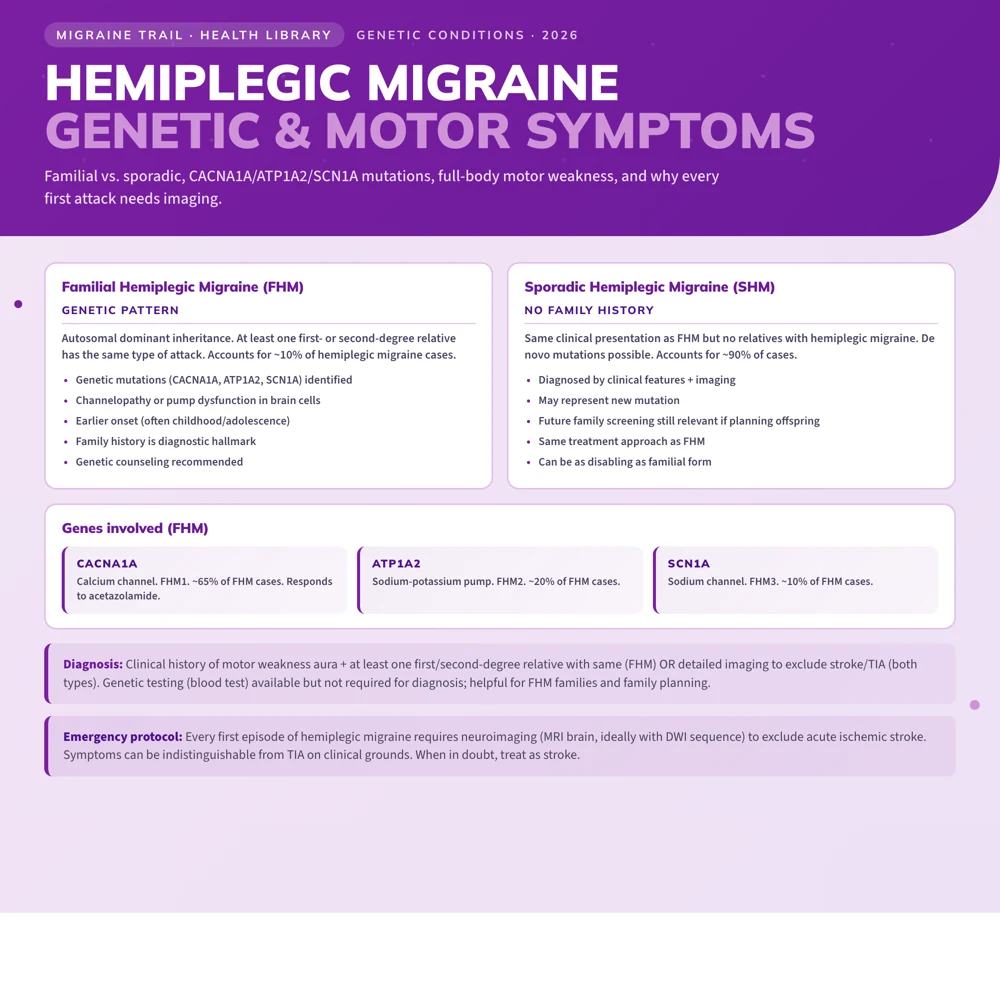
- Familial Hemiplegic Migraine (FHM): Autosomal dominant inheritance. At least one first- or second-degree relative has had attacks with motor aura. Three genetic subtypes (FHM1, FHM2, FHM3) are linked to specific gene mutations.
- Sporadic Hemiplegic Migraine (SHM): Identical clinical presentation but no family history of motor aura. It may represent new mutations, incomplete penetrance, or unrecognized family history.
Symptoms
Aura Phase
The aura in hemiplegic migraine is prolonged, typically lasting 1 hour to several days, far longer than the 5 to 60-minute visual aura of typical migraine. Symptoms develop gradually, often with a characteristic march: spreading from one body part to the next over time.
Motor symptoms (required for diagnosis):
- Hemiparesis: weakness on one side (arm, leg, face, or any combination)
- Hemiplegia: complete paralysis on one side (less common)
- The weakness may range from mild (difficulty gripping, a slight drag when walking) to profound (unable to lift the arm or stand)
- The side affected can vary from attack to attack
Sensory symptoms (very common):
- Unilateral tingling, numbness, or pins and needles
- Typically spreads from fingers up the arm, or from foot up the leg
Visual symptoms:
- Zigzag lines (fortification spectra)
- Blind spots (scotoma)
- Flickering vision
- Visual disturbances may affect one or both sides of the visual field
Speech disturbance (common):
- Dysarthria: slurred speech, difficulty forming words
- Aphasia: difficulty finding or producing words
- These symptoms are deeply frightening and can feel isolating when it becomes hard to communicate what is happening
Altered consciousness (in some cases):
- Confusion or disorientation
- Drowsiness
- In severe attacks: a coma-like state (rare, associated with FHM1 CACNA1A mutations)
Headache: A migraine headache typically follows the aura, though in some attacks the headache is mild or absent. The headache is often on the opposite side from the weakness.
Typical Attack Sequence
- Prodrome: yawning, mood changes, food cravings in the hours before
- Aura begins: usually visual symptoms first, then sensory spread, then motor weakness
- Motor weakness develops: often over 20 to 60 minutes, may worsen for several hours
- Headache phase: begins as aura is peaking or starting to resolve
- Aura resolves: motor weakness typically resolves fully within 24 hours, though some attacks have weakness lasting days to weeks
- Postdrome: fatigue, cognitive fog, vulnerability
What Causes Hemiplegic Migraine
Genetic Mutations (FHM)
Three genes account for the identified cases of familial hemiplegic migraine:
FHM1 (CACNA1A, a calcium channel gene): Mutations in this gene are found in approximately 50% of FHM families. FHM1 is associated with the most severe presentations, including prolonged hemiplegia, cerebellar ataxia between attacks, and rare coma episodes.
FHM2 (ATP1A2, the sodium-potassium pump): Mutations affecting this pump account for roughly 20% of FHM families.
FHM3 (SCN1A, a sodium channel gene): Rarer; accounts for a small percentage of FHM families.
Together these three genes account for about 70 to 80% of familial cases. The remaining 20 to 30% have unknown genetic causes, suggesting more genes are involved.
Mechanism
All three gene mutations affect the regulation of ion channels and pumps that control neuronal excitability. The result is a brain that is hyperexcitable, with a lower threshold for cortical spreading depression (CSD): the slow wave of electrical activity that underlies migraine aura.
In hemiplegic migraine, CSD spreads into the motor cortex and sometimes brainstem structures controlling motor function, producing the weakness that distinguishes it from typical migraine with aura.
Hemiplegic Migraine vs. Stroke: How to Tell Them Apart
This distinction is clinically critical and often cannot be made with certainty in an acute setting, which is why emergency evaluation for a first episode is so important and should never feel like an overreaction.
| Feature | Hemiplegic Migraine | Stroke or TIA | |---|---|---| | Onset of weakness | Gradual spread over minutes | Often sudden, maximal at onset | | Associated headache | Usually yes (may follow weakness) | May or may not have headache | | Visual symptoms | Often precede weakness | May occur simultaneously | | Sensory march | Common | Uncommon | | Prior similar episodes | Usually yes (after first attack) | Less likely | | Family history | Often present (FHM) | Cardiovascular risk factors | | Age | Often younger, first episodes in adolescence or young adulthood | All ages, higher in older adults | | Resolution | Typically complete within hours to days | May be partial or incomplete |
The most important thing to know: you cannot reliably distinguish hemiplegic migraine from stroke clinically during a first attack. Emergency evaluation is always the right call.
Diagnosis
When to Go to the Emergency Room
For any first episode of sudden weakness, facial drooping, speech disturbance, or severe headache, call emergency services. Do not wait to see if it resolves.
For people with established hemiplegic migraine, go to the ER if:
- The attack is significantly more severe or prolonged than usual
- Neurological deficits are not resolving on the expected timeline
- You are experiencing new symptoms that haven't occurred before
- Severe vomiting is causing dehydration
Diagnostic Workup
- MRI brain with DWI: the essential scan; diffusion-weighted imaging detects acute ischemia within minutes of onset. A normal DWI during an acute hemiplegic attack strongly supports migraine over stroke.
- MRA (MR angiography): to evaluate cerebral vasculature if arterial dissection or AVM is suspected
- EEG: if seizure is in the differential (some FHM presentations can include seizure activity)
- Genetic testing: CACNA1A, ATP1A2, SCN1A sequencing when FHM is suspected; useful for confirming diagnosis and guiding family discussions
- Detailed family history: a pattern of similar episodes in relatives is diagnostically important
Neurological examination between attacks is typically normal, though cerebellar signs may be present in FHM1 patients.
IHS Diagnostic Criteria
Familial hemiplegic migraine requires:
- Attacks meeting criteria for migraine with aura
- Aura includes fully reversible motor weakness
- At least one first- or second-degree relative has had attacks with motor aura
- Not better accounted for by another diagnosis
Sporadic hemiplegic migraine: Same criteria, without the family history requirement.
Treatment
Acute Treatment
Triptans and ergotamines are generally avoided in hemiplegic migraine due to theoretical vasoconstriction concerns, though the evidence that they cause harm is largely theoretical. Most guidelines currently recommend caution until better data is available.
First-line acute options:
- NSAIDs: ibuprofen 600 to 800mg, naproxen 500 to 1000mg, or ketorolac IM for severe attacks; starting at the first symptom gives the best chance of interrupting the attack
- Antiemetics: prochlorperazine or metoclopramide for nausea; prochlorperazine also reduces headache
- Gepants (ubrogepant, rimegepant): CGRP receptor antagonists that work without vasoconstriction, and are increasingly used in hemiplegic migraine
- IV fluids and IV ketorolac in the ER for severe attacks
For prolonged motor aura: Some specialists use intranasal or IV ketamine for severe prolonged hemiplegic attacks. There is case report evidence that it can abort the CSD underlying the aura.
Preventive Treatment
Because attacks are both disabling and frightening, preventive therapy is strongly recommended for hemiplegic migraine if attacks occur more than once or twice per year.
Calcium channel blockers (first-line):
- Verapamil (120 to 480mg/day): the most commonly used option; it affects the same calcium channels implicated in FHM1
- Flunarizine: not available in the US but widely used in Europe; strong evidence in migraine generally and specifically in FHM
Other preventives:
- Valproate (sodium valproate): effective; avoid in women of childbearing age without contraception (teratogenic)
- Lamotrigine: particularly suited to aura-dominant hemiplegic migraine
- Acetazolamide: specifically supported in FHM1 (CACNA1A mutations); acts on ion transport
- Topiramate
- Tricyclics (amitriptyline, nortriptyline): helpful when sleep disruption or anxiety are prominent features
CGRP monoclonal antibodies: Erenumab, fremanezumab, and galcanezumab are increasingly used in hemiplegic migraine, though not specifically approved for this subtype. Accumulating observational data suggests significant benefit in reducing attack frequency.
Contraception Considerations
Combined oral contraceptives are contraindicated in hemiplegic migraine due to significantly elevated stroke risk. Progesterone-only methods (the mini-pill, implant, Mirena) are safe and worth discussing with your doctor or gynaecologist.
Living With Hemiplegic Migraine
Living with hemiplegic migraine is genuinely hard. The unpredictability of attacks, the impact on work and independence, and the anxiety that can build between episodes are all real and valid parts of this experience. Being proactive about your care, building a relationship with a neurologist who takes your condition seriously, and connecting with others who understand are all meaningful steps.
Driving
Hemiplegic migraine that causes altered consciousness, visual symptoms, or motor weakness during attacks may affect fitness to drive. Legal requirements vary by country. In the UK and many US states, drivers with conditions causing episodic neurological impairment must notify the driving authority and may be required to pause driving until attacks are controlled. Your neurologist can help guide this conversation and provide supporting documentation.
Workplace and Legal Documentation
Having a documented diagnosis and a letter from your neurologist explaining the condition is valuable for workplace accommodations, particularly if episodes have required emergency responses or significant time off work. You are entitled to support, and good documentation makes accessing it easier.
Trigger Management
Triggers for hemiplegic migraine are similar to general migraine triggers, but some are particularly common:
- Physical exertion: some people have attacks triggered by vigorous exercise or even minor head trauma
- Emotional stress
- Sleep disruption
- Hormonal changes: particularly around menstruation
Track every attack carefully, including date, duration, symptoms, preceding activities, and potential triggers. This data guides preventive treatment decisions and helps establish the pattern needed for specialist management.
Use Migraine Trail to log full attack details by voice, track aura symptoms specifically, and generate structured PDF reports for your neurologist. That level of detail is essential for the kind of careful temporal analysis hemiplegic migraine requires.