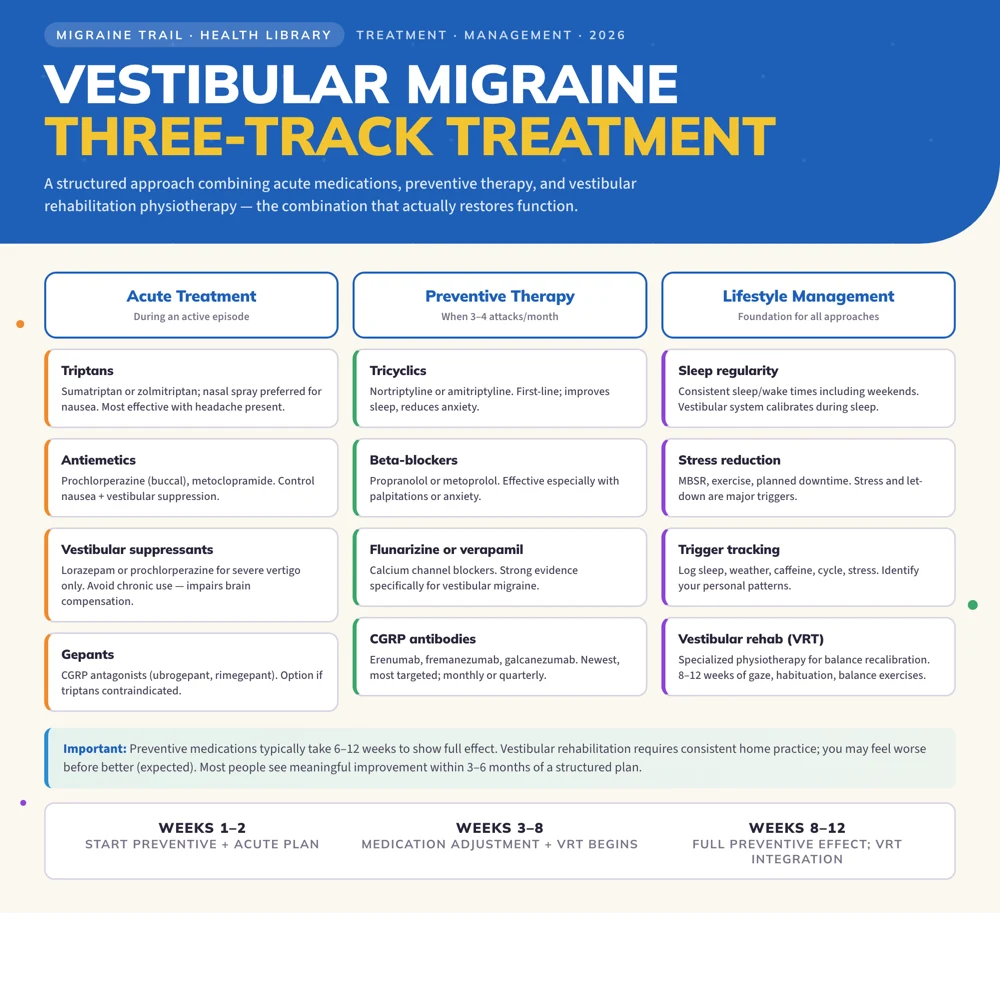
Vestibular migraine treatment follows a three-track approach: acute medications for active episodes (triptans, antiemetics, vestibular suppressants), preventive therapy to reduce episode frequency (tricyclics, beta-blockers, CGRP antibodies), and vestibular rehabilitation physiotherapy to rebuild balance function and reduce motion sensitivity. Lifestyle management, particularly sleep, stress, and trigger tracking, is foundational and often produces substantial improvement on its own.
Living with vestibular migraine can be disorienting in every sense of the word. The dizziness, vertigo, and unsteadiness do not just affect your balance; they can make you afraid to drive, anxious in busy places, and exhausted from constantly compensating for a visual world that won't stay still. Many people with vestibular migraine spend years being told they have an inner ear problem, or anxiety, or simply vertigo of unknown cause, before the connection to migraine is finally made.
If you have recently received a diagnosis of vestibular migraine, or suspect you may have it, there is real reason for hope. A structured treatment plan dramatically improves quality of life for most people. This article covers treatment in full detail. For an overview of symptoms, diagnosis, and differential diagnosis, see the vestibular migraine guide.
Acute Treatment: Stopping an Active Episode
Vestibular migraine episodes vary from minutes to 72 hours. Acute treatment is most effective when taken at the very onset of symptoms, so having your medications accessible and a plan ready matters.
Triptans
Triptans are the evidence-backed first choice for acute migraine treatment and are increasingly supported for vestibular migraine specifically. Sumatriptan and zolmitriptan have the most data in vestibular migraine; nasal spray formulations of both are particularly useful because nausea and vomiting may prevent oral absorption.
Best option when: The episode includes headache alongside vestibular symptoms. Evidence for triptan effect on isolated vertigo without headache is less consistent.
Contraindications: Cardiovascular disease, uncontrolled hypertension, hemiplegic migraine, basilar-type migraine (discuss with your neurologist).
Antiemetics
Nausea and vomiting are prominent in vestibular migraine episodes. Antiemetics both control nausea and have direct vestibular and headache benefits:
- Prochlorperazine: strong antiemetic with vestibular suppression; available as a buccal tablet (dissolves inside the cheek, bypassing swallowing when that is difficult)
- Metoclopramide: useful for nausea; also speeds absorption of orally co-administered medications
- Ondansetron: effective for vomiting control; less effect on headache itself
Vestibular Suppressants
For episodes dominated by vertigo and dizziness with minimal headache, vestibular suppressants provide symptomatic relief:
- Lorazepam (0.5 to 1mg): effective for severe vertigo; use sparingly, as benzodiazepines suppress the brain's compensation process if used repeatedly
- Prochlorperazine: doubles as antiemetic and vestibular suppressant
- Meclizine (Antivert): over-the-counter antihistamine with mild vestibular suppression; less effective than benzodiazepines but safer for repeated use
Important: Vestibular suppressants should be used only for acute severe episodes, not taken daily or preventively. Chronic use impairs the brain's ability to compensate and can actually perpetuate ongoing dizziness between attacks. This is a well-known trap that is easy to fall into when dizziness feels constant.
Gepants (CGRP Antagonists)
Ubrogepant and rimegepant are CGRP receptor antagonists approved for acute migraine. Growing evidence suggests CGRP is involved in vestibular migraine pathophysiology, making gepants a promising option, particularly for people who cannot tolerate triptans due to cardiovascular contraindications.
Preventive Treatment: Reducing Episode Frequency
Preventive therapy is worth discussing when vestibular migraine episodes are:
- Occurring more than 3 to 4 times per month
- Significantly disabling (affecting ability to drive, work, or function)
- Prolonged (lasting many hours per episode)
- Not adequately controlled by acute treatment
All vestibular migraine preventive options are extrapolated from general migraine prevention trials, as there are no large randomized controlled trials specifically for vestibular migraine prevention. However, observational studies and extensive clinical experience consistently support benefit.
Tricyclic Antidepressants (First-Line)
Nortriptyline or amitriptyline (10 to 75mg at night) are widely used as first-line preventive therapy for vestibular migraine. Benefits include:
- Evidence base in migraine and vestibular migraine specifically
- Also improves sleep quality (disrupted sleep is a major trigger)
- Addresses anxiety and depression, which frequently co-occur with vestibular conditions
- Low cost
Side effects include morning drowsiness, dry mouth, constipation, and weight gain. Starting at the lowest effective dose (10mg) and titrating slowly minimizes these. It can take 4 to 6 weeks to see the full benefit.
Beta-Blockers
Propranolol (40 to 120mg/day) or metoprolol are standard first-line migraine preventives with consistent benefit in vestibular migraine. Propranolol is particularly useful when palpitations or anxiety are prominent features.
Avoid in: Asthma, significant bradycardia, peripheral vascular disease, depression (can worsen).
Venlafaxine (SNRI)
Venlafaxine (37.5 to 150mg) is particularly popular for vestibular migraine in people with comorbid anxiety, a very common combination. Some neurologists use it as first-line specifically when anxiety is prominent. Evidence is positive, though from smaller studies.
Calcium Channel Blockers
Flunarizine (5 to 10mg) is not available in the US but is widely used in Europe and Canada. It is one of the strongest-evidenced preventives for vestibular migraine specifically. Verapamil is used where flunarizine is not available.
Topiramate
Topiramate (25 to 100mg/day) is an effective migraine preventive with reasonable evidence in vestibular migraine. Cognitive side effects known as "topamax fog" (word-finding difficulty, concentration problems) are dose-dependent and troublesome for some people. Starting very low (12.5mg) and increasing slowly reduces this risk.
CGRP Monoclonal Antibodies
Erenumab, fremanezumab, galcanezumab are monthly or quarterly injections blocking the CGRP pathway. These are the newest and most targeted preventive class. Evidence in vestibular migraine is accumulating:
- A growing number of case series and observational studies show significant reduction in both headache and vestibular episodes
- Better tolerated than older preventives, with minimal systemic side effects
- Expensive; insurance coverage typically requires documented failure of other preventives first
For people with frequent, disabling vestibular migraine who have not responded to 2 to 3 other preventives, CGRP antibodies are increasingly being recommended. They may be worth pushing for if other options have not worked.
Vestibular Rehabilitation Therapy (VRT)
Vestibular rehabilitation is a specialized form of physiotherapy targeting the balance system. If you experience any of the following between attacks, VRT may help significantly:
- Persistent imbalance or unsteadiness that does not fully resolve
- Motion sensitivity or visually induced dizziness in everyday situations
- A chronic "rocking," floating, or unsteady sensation
- Difficulty in visually complex environments (supermarkets, crowds, busy roads)
VRT provides exercises designed to promote central compensation: the brain's process of recalibrating its reliance on conflicting vestibular, visual, and proprioceptive signals. It does not treat the migraine itself, but it can dramatically improve the quality of your life between attacks.
What VRT Involves
A vestibular physiotherapist typically prescribes a home exercise program including:
- Gaze stabilization exercises: moving the head while keeping focus on a target; retrains the vestibulo-ocular reflex
- Habituation exercises: repeated exposure to movement or visual environments that trigger dizziness, at a level that produces mild discomfort without overwhelming; reduces hypersensitivity over time
- Balance training: standing on unstable surfaces, walking with head movements, gradually reducing reliance on visual input for balance
- Graded exposure to visual environments: starting with simple visual scenes, progressing to busier ones
What to Expect
VRT requires consistency over 6 to 12 weeks. The exercises will initially provoke mild dizziness. This is expected and is necessary for the compensation process to occur. Many people feel worse before they feel better, and that can be discouraging. Patients who stop when the exercises feel uncomfortable unfortunately do not get the benefit.
Having a good vestibular physiotherapist who can adjust your program based on your response makes a real difference. If the exercises are significantly worsening your symptoms for more than a day or two, tell your therapist; the program may need to be modified.
Find a physiotherapist with specific vestibular rehabilitation certification. In the US, look for Emory VR certification or similar specialist credentials.
Lifestyle Management
Lifestyle factors often make the difference between well-controlled and poorly-controlled vestibular migraine. The vestibular system is particularly sensitive to the same triggers that worsen migraine generally, and it responds well to consistency.
Sleep Regularity
Vestibular migraine episodes frequently follow nights of poor sleep or disrupted sleep schedules. Maintaining consistent sleep and wake times, including on weekends, is one of the most powerful single interventions. The vestibular system is calibrated during sleep; disruption leads to instability. This is not always easy when life is busy or unpredictable, but even partial consistency helps.
Stress Management
Stress is a major trigger for vestibular migraine specifically. Many people notice vestibular episodes clustering after periods of high stress, particularly during the "let-down" period afterward. Mindfulness-based stress reduction (MBSR), regular aerobic exercise, and planned downtime help prevent stress accumulation. If stress is a consistent trigger, that is worth addressing directly, not as a character issue but as a medical management strategy.
Dietary Factors
Common dietary triggers for vestibular migraine include caffeine (especially withdrawal), alcohol (particularly wine and beer), aged cheeses, processed meats, and artificial sweeteners. Keeping blood sugar stable with regular meals is particularly important; many people with vestibular migraine are sensitive to hypoglycemia, and skipping meals can precipitate episodes.
Caffeine Management
Caffeine withdrawal is a potent vestibular migraine trigger. If you consume caffeine daily, maintain a consistent dose and timing rather than cutting it out abruptly. If you want to reduce your intake, do it very gradually (around 10 to 20% per week) to avoid triggering an attack.
Trigger Tracking
Because vestibular migraine episodes often have multiple interacting triggers, tracking helps identify your personal pattern. Common migraine triggers apply, but the vestibular system also responds to:
- Hormonal changes: menstrual cycle timing is often a dominant trigger
- Barometric pressure drops: weather changes before storms
- Visual overload: extended screen time, certain visual environments
- Dehydration: even mild dehydration worsens vestibular function
Track episodes alongside sleep data, weather, hormonal cycle, dietary intake, and stress levels using Migraine Trail. The app automatically overlays weather data with your attack log. For many people with vestibular migraine, seeing the weather-episode correlation visually for the first time is a revelation that transforms how they understand their condition.
Getting the Right Specialist
Vestibular migraine is best managed by a neurologist, ideally one with headache or vestibular neurology expertise. In many health systems, the pathway involves:
- GP: initial diagnosis, basic lifestyle advice, first-line preventive trial
- Neurologist: confirmed diagnosis, comprehensive preventive management
- ENT or audiovestibular physician: if there is genuine diagnostic uncertainty about Menière's disease
- Vestibular physiotherapist: for VRT alongside medical management
For a neurologist appointment, bring a detailed log of all episodes showing date, duration, vestibular symptoms, headache features, associated symptoms, and triggers. A six-week diary from Migraine Trail as a PDF report gives a specialist far more usable information than verbal recall alone, and can significantly accelerate getting to the right treatment plan.
How Long Does Treatment Take?
Preventive medications typically take 6 to 12 weeks to show full effect. Vestibular rehabilitation takes 8 to 12 weeks of consistent exercise. Most people with vestibular migraine see significant improvement within 3 to 6 months of a structured treatment plan, but patience is genuinely required.
The goal of treatment is not complete cure, but meaningful functional improvement: fewer episodes, milder episodes, shorter recovery, and the ability to be in environments that were previously impossible or exhausting. Many people find they gradually regain parts of their life they thought they had lost to this condition. That progress is real, and it is worth working toward.