A migraine cocktail is an intravenous (IV) combination of medications given in the emergency room for severe or refractory migraine. The standard protocol typically includes an antiemetic (prochlorperazine or metoclopramide), an NSAID (ketorolac, also known as Toradol), IV fluids for rehydration, and often magnesium sulfate. Diphenhydramine (Benadryl) is frequently added to prevent restlessness from the antiemetic. Dexamethasone is often included to prevent early relapse. The combination works by simultaneously targeting multiple migraine pathways: nausea, neuroinflammation, vascular changes, and CGRP activity.
Ending up in the emergency room with a migraine can be frightening and demoralizing. You may feel like you failed at managing your condition, or worry that staff will not take your pain seriously. Neither of those things is true. When a migraine crosses the line into severe, intractable, or lasting more than 72 hours, the ER is exactly the right place to be. The migraine cocktail exists precisely because some attacks are too big to manage at home, and there is no shame in needing it.
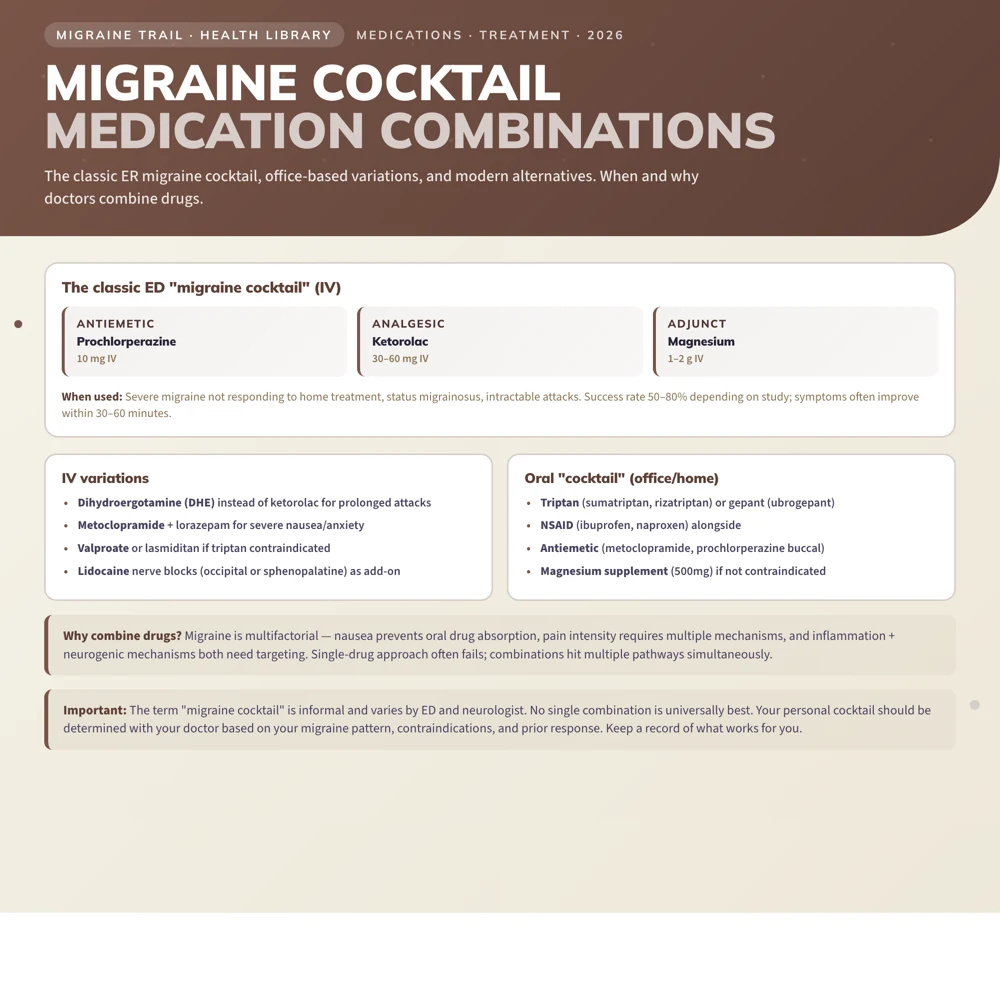
The term "migraine cocktail" is informal. There is no single standardized formula. Emergency departments vary in their exact protocols, and the composition may be adjusted based on individual patient history, contraindications, and response. What the various protocols share is a core principle: target migraine from multiple angles simultaneously rather than relying on one medication to do all the work.
When Is a Migraine Cocktail Used?
A migraine cocktail is the standard ER treatment for:
- Status migrainosus: a migraine lasting more than 72 hours that has not responded to home treatment
- Intractable migraine: a severe attack that has not responded to oral rescue medications at home
- Migraine with severe vomiting: when you cannot keep oral medications down
- Migraine with significant dehydration: when IV fluids are needed regardless of which medications are chosen
- Breakthrough migraine: a severe attack in someone who normally manages well, but whose usual regimen has failed this time
If you are wondering whether to go to the ER, the key indicators are: migraine lasting more than 72 hours, inability to keep down fluids or medications, and failure of all home rescue options. See the full guide to intractable migraine and status migrainosus.
The Medications in a Migraine Cocktail
1. Antiemetic (First Priority)
Prochlorperazine (Compazine) or Metoclopramide (Reglan)
Antiemetics are the cornerstone of the ER migraine protocol, not just for nausea control, but because they have direct headache-relieving properties through dopamine receptor blockade in the brainstem.
Multiple emergency medicine trials have shown prochlorperazine and metoclopramide are as effective as ketorolac (the IV NSAID) for migraine headache relief, and more effective than opioids. Prochlorperazine has slightly stronger evidence, but both are well-established.
Standard doses:
- Prochlorperazine: 10mg IV
- Metoclopramide: 10mg IV
Important: Both can cause akathisia, an intensely uncomfortable inner restlessness and urge to move that affects roughly 20 to 40% of patients. This side effect is managed by pre-treating with diphenhydramine (Benadryl) 25mg IV, which is why Benadryl is nearly always part of the protocol. If you experience akathisia during treatment, tell the nurse immediately. It can be treated quickly.
2. Diphenhydramine (Benadryl)
25 to 50mg IV
Diphenhydramine is included primarily to prevent akathisia from the antiemetic. It also has mild sedative and antiemetic properties. Some ER protocols omit it if using an antiemetic with lower akathisia risk (like ondansetron), but it remains standard when prochlorperazine or metoclopramide are used.
3. Ketorolac (Toradol) — IV NSAID
15 to 30mg IV or IM
Ketorolac is an NSAID that cannot be taken orally in effective doses; it is only available as an injection. It provides strong anti-inflammatory effects through COX inhibition, targeting the neurogenic inflammation that drives migraine pain.
Ketorolac is significantly more effective for migraine than oral ibuprofen or naproxen taken at home, due to faster, more complete absorption via the IV route and higher effective tissue concentration.
Contraindications: Aspirin allergy, active peptic ulcer, renal impairment, bleeding disorders, pregnancy.
4. IV Fluids
Normal saline 500 to 1000ml
Most people arriving at the ER with a severe migraine have been unable to eat or drink normally, often combined with vomiting. Dehydration worsens migraine: low blood volume and reduced cerebral perfusion both contribute to pain and medication non-response.
IV fluids serve multiple purposes: rehydration, a vehicle for delivering other medications, and a direct effect on headache through improved cerebral blood flow. There is also evidence that the experience of receiving IV treatment in a calm clinical setting contributes meaningfully to response rates in migraine. Sometimes being looked after is itself therapeutic.
5. Magnesium Sulfate
1 to 2g IV over 15 to 30 minutes
IV magnesium has consistent evidence in migraine treatment, particularly for:
- Migraine with aura: strong evidence; magnesium deficiency is prevalent in people with migraine and aura is particularly responsive
- Menstrual migraine
- Migraine refractory to other medications
Magnesium works through several mechanisms: blocking NMDA receptors (reducing cortical excitability), inhibiting cortical spreading depression, and reducing CGRP release. Many people with migraine have chronically low magnesium levels, and supplementation, both IV acute and oral preventive, is well-supported.
Magnesium is safe, inexpensive, and well-tolerated. You may feel a warm flush during the infusion, which is normal.
6. Dexamethasone (Corticosteroid)
10 to 25mg IV, single dose
Dexamethasone does not provide immediate pain relief; it takes hours to act. Its role in the migraine cocktail is specifically to prevent early headache recurrence within 24 to 72 hours after ER discharge.
Multiple randomized controlled trials show that adding a single IV dose of dexamethasone significantly reduces the rate of headache returning within 72 hours compared to placebo. This is particularly valuable for people who find that their migraine comes back the next day after being treated, a pattern that is both exhausting and demoralizing.
Other Medications Sometimes Included
Sumatriptan SC: If you have not tried triptans during this attack, subcutaneous sumatriptan (6mg) may be given in the ER, bypassing oral absorption issues and providing rapid CGRP pathway blockade.
DHE (Dihydroergotamine): IV or IM DHE is used for attacks that have not responded to the standard protocol. It is highly effective but requires ECG monitoring and is contraindicated in cardiovascular disease, recent triptan use, and pregnancy. DHE is often a "rescue within the rescue" for truly refractory attacks.
Valproate IV: Occasionally used in specialist settings for severe refractory attacks.
Opioids: Despite widespread historical use, opioids (morphine, hydromorphone) are now not recommended for migraine in most guidelines. They are less effective than antiemetics and NSAIDs, cause significant nausea, and can worsen long-term migraine frequency. Emergency medicine guidelines increasingly state explicitly that opioids should not be first-line for migraine. If you are offered opioids in the ER and would prefer the evidence-based protocol, you are within your rights to ask for it.
What to Expect During Treatment
The typical ER migraine treatment experience:
- Triage and assessment: history, vitals, and IV line placed
- Medications administered: usually IV push or short infusion over 15 to 30 minutes
- Monitoring period: 1 to 2 hours in the department to assess response and watch for akathisia or allergic reaction
- Response: most people experience significant improvement within 45 to 90 minutes; pain-free rates at 2 hours in clinical trials are typically 50 to 70%
- Discharge: with oral medications for home (a short steroid course, updated rescue plan) and follow-up instructions
- Relapse risk: without dexamethasone, up to 40% of patients experience headache return within 24 to 72 hours; with dexamethasone this is significantly reduced
After the ER: What Comes Next
Receiving a migraine cocktail in the ER is a signal that your current management plan needs to be updated, not a sign of weakness or failure. After discharge, follow up with your GP or neurologist to:
- Review why home rescue medications failed this time
- Consider starting or adjusting preventive therapy
- Develop a written escalation plan so you know exactly what to take, in what order, and at what point to go to the ER
- Evaluate for medication overuse if frequent acute treatment use was a factor
Having a plan written down before the next bad attack is one of the most compassionate things you can do for yourself. Making complex decisions mid-attack, when you are in severe pain and possibly vomiting, is genuinely hard. A plan removes that burden.
Track your attack patterns, medication use, and trigger exposures with Migraine Trail. The longitudinal data, including attack frequency, severity trends, and medication use per month, is exactly what a neurologist needs to make informed decisions about whether preventive therapy is warranted and what type would work best for you.