An intractable migraine is one that does not respond to standard treatments and lasts longer than 72 hours. This is called status migrainosus. It requires emergency medical care, typically involving IV medications including antiemetics, NSAIDs, magnesium, and sometimes corticosteroids. If your migraine has lasted more than three days or your usual medications have stopped working, please go to the emergency room.
There is a particular despair that comes with a migraine that simply won't end. You've tried everything you have at home. You've lain in the dark, tried to sleep, taken your medications, and the pain keeps returning or never leaves. After two or three days of this, many people feel broken. They wonder if something has gone permanently wrong, or if they are somehow not managing their condition well enough.
Status migrainosus is not a failure of willpower. It is a distinct neurological condition that requires medical intervention, and going to the emergency room is the right response, not an overreaction.
What Is Status Migrainosus?
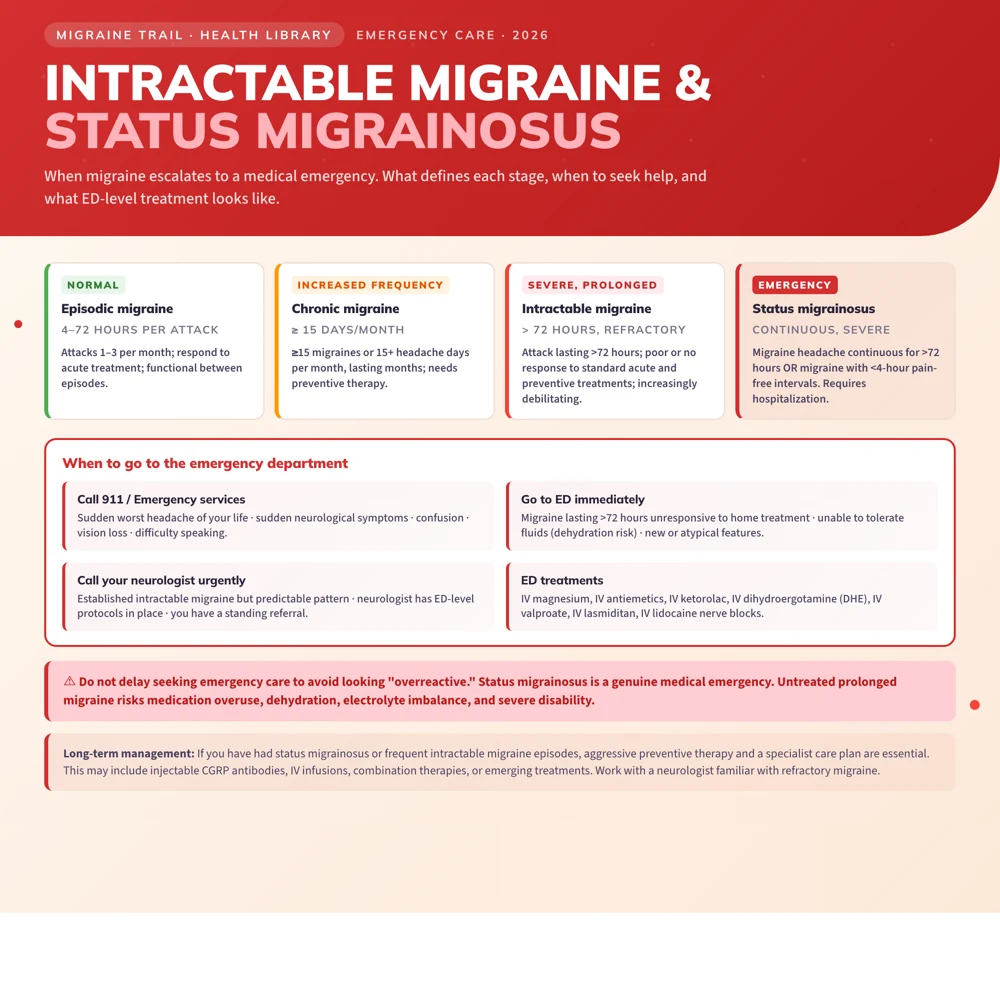
Status migrainosus is defined by the International Headache Society as a migraine attack lasting more than 72 hours (3 days), with headache intensity that is debilitating, and that is not adequately controlled by standard oral medications.
The term intractable migraine is used more loosely to describe any migraine that is refractory, meaning it does not respond to the treatments you would normally take. An intractable migraine may or may not have crossed the 72-hour threshold.
Both share a common feature: the normal rescue medications have failed. The migraine has become a medical problem that cannot be solved at home.
Symptoms
Status migrainosus looks like a severe migraine episode that has simply refused to end:
- Continuous or near-continuous head pain lasting beyond 72 hours
- Pain that is moderate to severe, often throbbing or pulsating
- Nausea and vomiting, sometimes severe enough to cause dehydration
- Extreme light and sound sensitivity
- Inability to function normally: to work, care for children, eat, or sleep
- In some cases, neurological symptoms such as difficulty concentrating, visual disturbances, or confusion
Unlike typical migraines that have distinct phases, status migrainosus may feel like one unbroken wave of pain, or it may cycle: partially improving, then worsening, without ever fully resolving. The exhaustion and disorientation that builds over days like this is its own kind of suffering.
Risks of Untreated Status Migrainosus
Leaving status migrainosus untreated is not safe:
- Severe dehydration from prolonged vomiting and inability to keep fluids down
- Medication overuse: in desperation, people may take escalating doses of pain relievers, which can worsen the cycle
- Stroke risk: prolonged migraines with aura are associated with increased ischemic stroke risk, particularly in women who smoke or use hormonal contraceptives
- Persistent neurological changes: a rare complication called migrainous infarction can occur when aura symptoms become permanent due to reduced blood flow
When to Go to the Emergency Room
Please go to the ER if:
- Your migraine has lasted more than 72 hours
- Your usual rescue medications have completely stopped working
- You are vomiting and cannot keep down fluids or oral medications
- The headache is the worst of your life or came on with sudden, explosive onset (sometimes called a "thunderclap" headache)
- You have new neurological symptoms: weakness on one side, slurred speech, sudden vision loss, confusion
- You have a fever with the headache (which may suggest meningitis)
A thunderclap headache or sudden worst-ever headache is a medical emergency regardless of your history with migraine. It can indicate a subarachnoid hemorrhage and requires immediate evaluation.
You are not being dramatic. You are doing the right thing.
ER and Hospital Treatment for Intractable Migraine
Emergency treatment targets multiple pathways at once. The typical IV protocol includes:
Antiemetics (First Priority)
- Prochlorperazine (Compazine): the most studied and effective first-line ER antiemetic for migraine; it also has direct headache benefit
- Metoclopramide (Reglan): similar mechanism; often given with diphenhydramine (Benadryl) to prevent akathisia (an uncomfortable inner restlessness)
- Ondansetron (Zofran): used more for nausea control than headache relief
NSAIDs
- Ketorolac (Toradol): IV or IM NSAID, highly effective when oral NSAIDs have failed; reduces the inflammation contributing to the attack
Magnesium Sulfate
- IV magnesium at 1 to 2g over 15 to 30 minutes is commonly used, particularly for migraine with aura; evidence supports benefit in aura and overall attack termination
Triptans
- If not already tried, subcutaneous sumatriptan may be administered in the ER; oral triptans are often skipped given the likelihood that previous oral triptan attempts have already failed
Corticosteroids
- A single dose of dexamethasone (10 to 25mg IV) is often given alongside other treatment to reduce the risk of early relapse within 24 to 72 hours of discharge; it does not provide immediate pain relief but appears to prevent the migraine from returning the next day
DHE (Dihydroergotamine)
- IV or IM DHE is used for intractable cases that have not responded to the above; it is highly effective but requires monitoring for side effects and is contraindicated in cardiovascular disease
IV Fluids
- Rehydration is a standard part of ER management, particularly when vomiting has been prolonged
The combination most commonly used, antiemetic, ketorolac, magnesium, and IV fluids, with optional dexamethasone for relapse prevention, is sometimes informally called a migraine cocktail, though the exact composition varies by hospital and provider. See the full migraine cocktail guide.
What Happens After the ER
Leaving the ER is not the end of the story. After a severe attack like status migrainosus, the risk of relapse is significant, and the management plan that got you here needs to change. Standard discharge planning includes:
- A short course of oral corticosteroids (prednisolone or dexamethasone) to prevent rebound
- Review of your rescue medication: what you had at home was not enough, and your team needs to know that
- Referral to neurology if you are not already under specialist care
- A conversation about preventive treatment: status migrainosus is a strong signal that daily preventive therapy needs to be discussed
Please advocate for yourself if these things are not offered. You have had a serious neurological event, and you deserve a proper follow-up plan.
Preventive Treatment After Status Migrainosus
A single episode of status migrainosus is a warning that something in the migraine management plan needs to change. In the weeks following, a neurologist will typically:
- Review and initiate or revise preventive therapy: topiramate, propranolol, amitriptyline, or CGRP monoclonal antibodies
- Assess for medication overuse headache, which often co-occurs and perpetuates the cycle
- Develop a written rescue plan specifying what to take, in what order, and when to go to the ER, so you do not have to make that decision mid-attack when you are in severe pain
Preventing Status Migrainosus
The best way to avoid status migrainosus is careful management of ordinary migraine attacks before they escalate:
- Treat early: Take rescue medication at the first sign of an attack, not after hoping it will pass
- Avoid medication overuse: Taking acute migraine treatments more than 10 to 15 days per month can paradoxically worsen headache frequency
- Track your attacks: Identifying patterns in your migraine data allows you and your neurologist to catch escalating frequency before it becomes a crisis
- Have an escalation plan written down: Know in advance what step 1, step 2, and "go to the ER" look like for you, so you are not making that decision in the middle of a severe attack
Use Migraine Trail to track attack duration, medication use, and severity over time. That data gives your neurologist exactly what they need to adjust your treatment plan before the next severe attack.