Migraine without aura is the most common form of migraine, accounting for approximately 75% of all migraine diagnoses. It is defined by recurrent headache attacks lasting 4 to 72 hours with at least two of four features: unilateral location, pulsating quality, moderate-to-severe intensity, and worsening with routine activity, plus nausea, vomiting, or sensitivity to light and sound. Unlike migraine with aura, there are no warning neurological symptoms preceding the headache.
If you have migraine without aura, you may have spent years wondering whether what you experience is "really" migraine, because there are no dramatic visual symptoms to point to. You may have been told it sounds like a tension headache, or been dismissed by someone who assumed migraine always comes with warning zigzags. It doesn't.
Migraine without aura is just as disabling, just as real, and just as deserving of proper treatment as any other migraine type. In fact, because it lacks the obvious warning of visual aura, it can be harder to manage and easier to overlook. You deserve clarity about what you are dealing with.
What Is Migraine Without Aura?
Migraine without aura (previously called "common migraine" or "hemicrania simplex") is classified by the International Headache Society as a distinct primary headache disorder. It runs in families, is driven by trigeminal nerve sensitization and cortical spreading depression, and involves neuroinflammatory processes that distinguish it fundamentally from tension-type headache, even when both cause head pain.
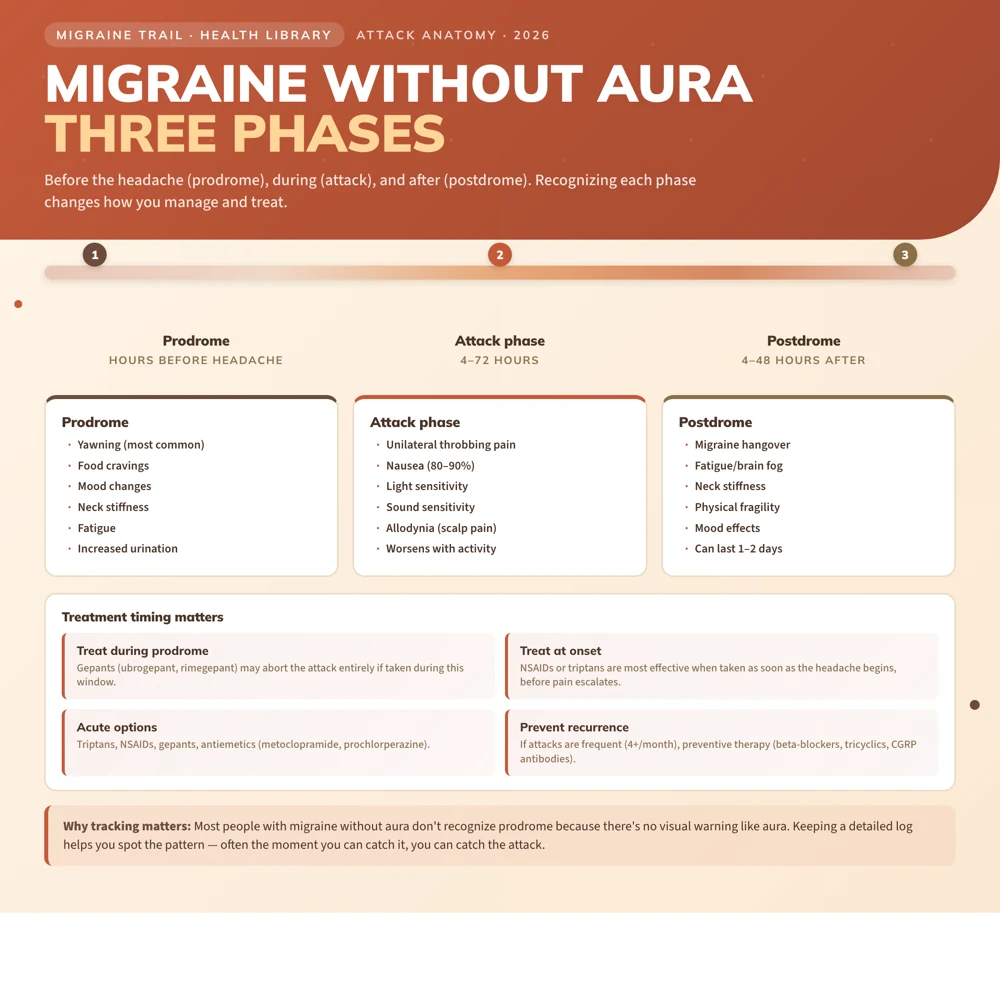
The absence of aura does not mean the attack appears without warning. Many people with migraine without aura experience premonitory symptoms (prodrome) in the hours before the headache begins: yawning, food cravings, neck stiffness, mood changes, or fatigue. These are easy to miss or attribute to something else, but learning to recognize them gives you a window to act early.
Diagnostic Criteria
The IHS ICHD-3 criteria for migraine without aura require:
A. At least 5 attacks fulfilling criteria B through D
B. Headache attacks lasting 4 to 72 hours (untreated or unsuccessfully treated)
C. Headache has at least 2 of the following 4 characteristics:
- Unilateral location (one side of the head)
- Pulsating quality (throbbing)
- Moderate or severe pain intensity
- Aggravation by or causing avoidance of routine physical activity (walking, climbing stairs)
D. During headache, at least 1 of the following:
- Nausea and/or vomiting
- Photophobia AND phonophobia (sensitivity to light and sound)
E. Not better accounted for by another ICHD-3 diagnosis
In practice, many people do not tick every box every time. Attacks can vary in character, location, and associated symptoms from episode to episode. This variability is itself characteristic of migraine, not evidence that it is "not really" migraine.
Symptoms in Detail
The Headache Phase
Pain in migraine without aura typically:
- Builds gradually from mild to moderate or severe over 30 to 90 minutes
- Is felt on one side of the head in about 60 to 70% of attacks, though bilateral attacks also occur
- Has a throbbing or pulsating quality synchronized with the heartbeat
- Lasts between 4 and 72 hours (attacks shorter than 4 hours or longer than 72 hours suggest reconsidering the diagnosis)
Associated Symptoms
- Nausea: present in 80 to 90% of attacks; sometimes severe enough to cause vomiting
- Photophobia: sensitivity to bright light; most people retreat to a dark room
- Phonophobia: sensitivity to sound; even normal conversation can feel intolerable
- Osmophobia: sensitivity to smells; present in many people with migraine and helpful diagnostically
- Allodynia: pain from normally non-painful stimuli, such as brushing hair, wearing glasses, or touching the scalp; develops during longer attacks as sensitization progresses
Prodrome (Before the Headache)
Up to 77% of people with migraine experience premonitory symptoms hours before the headache:
- Yawning (the most consistently reported)
- Food cravings (particularly for sweet foods)
- Mood changes: irritability, low mood, or sometimes euphoria
- Neck stiffness or soreness
- Fatigue or difficulty concentrating
- Increased urination
Recognizing prodrome is clinically important because treating during prodrome with gepants (ubrogepant, rimegepant) may prevent the headache phase from developing fully. Learning your own prodrome signals takes time, but it can genuinely change how you manage attacks.
Postdrome (After the Headache)
Once the headache resolves, a "migraine hangover" often follows for 4 to 48 hours: fatigue, cognitive difficulty (brain fog), neck stiffness, and a sense of physical fragility. This phase is real and can significantly extend the total impact of an attack beyond the headache itself.
Migraine Without Aura vs. Migraine With Aura
The key difference is the presence or absence of reversible neurological symptoms (aura) that precede or accompany the headache. In migraine with aura, people experience visual disturbances (zigzag lines, blind spots), sensory tingling, or less commonly speech or motor symptoms, lasting 5 to 60 minutes before the headache starts.
Important clinical distinction: Migraine with aura carries a higher risk of ischemic stroke, particularly in women who smoke or use combined oral contraceptives. This risk does not apply to migraine without aura. Treatment choices, particularly around hormonal contraception, may differ based on aura status. This is worth discussing explicitly with your doctor.
Many people have both types. About 20% of people with migraine have some attacks with aura and some without.
Migraine Without Aura vs. Tension-Type Headache
This is the most common diagnostic confusion, and it matters because the treatments are different. Key differences:
| Feature | Migraine Without Aura | Tension-Type Headache | |---|---|---| | Pain location | Often unilateral | Typically bilateral ("band") | | Pain quality | Throbbing or pulsating | Pressing or tightening | | Severity | Moderate to severe | Mild to moderate | | Activity effect | Worsened | Not worsened | | Nausea | Yes (diagnostic) | At most mild | | Light sensitivity | Yes | Mild or absent | | Duration | 4 to 72 hours | 30 minutes to 7 days |
In practice, the aggravation by activity and nausea criteria are the most distinguishing features. If climbing stairs makes the headache worse and you feel sick, it is almost certainly migraine.
If you have been told for years that you have tension headaches but the description above resonates, it is worth having a fresh conversation with your GP or a neurologist.
Triggers
Migraine without aura shares common migraine triggers with other forms:
- Sleep disruption: both sleep deprivation and oversleeping
- Hormonal fluctuations: perimenstrual migraine without aura is extremely common
- Stress: particularly the stress letdown effect (the weekend migraine pattern)
- Dietary factors: skipped meals, caffeine, alcohol (especially red wine)
- Weather changes: barometric pressure drops are well-documented triggers
- Dehydration
- Sensory stimuli: strong smells, bright lights, loud environments
Treatment
Acute Treatment
Mild to moderate attacks:
- NSAIDs (ibuprofen 400 to 600mg, naproxen 500mg, aspirin 900mg) taken early in the attack
- Combination analgesics: acetaminophen, aspirin, and caffeine combined (the combination has evidence comparable to triptans in mild to moderate attacks)
Moderate to severe attacks:
- Triptans (sumatriptan, rizatriptan, eletriptan, zolmitriptan): the gold standard for moderate-to-severe migraine; most effective when taken early; not suitable for people with cardiovascular disease
- Gepants (ubrogepant, rimegepant): CGRP receptor antagonists with good evidence; can be used in people who cannot take triptans; can also be used during prodrome to potentially abort the attack
- Lasmiditan (Reyvow): effective but causes sedation; not used if driving within 8 hours
- Ergotamines (DHE): less commonly used as first-line but effective for long attacks
Anti-nausea:
- Metoclopramide or prochlorperazine alongside analgesics: both reduce nausea and have direct headache benefit; metoclopramide also speeds absorption of oral medications
Preventive Treatment
Preventive therapy is worth discussing when attacks are frequent (4 or more per month), prolonged, severely disabling, or when acute treatments are failing or being overused. See the full guide to acute vs. preventive migraine treatment.
First-line preventive options include:
- Beta-blockers: propranolol, metoprolol
- Tricyclic antidepressants: amitriptyline, nortriptyline
- Anticonvulsants: topiramate, sodium valproate
- CGRP monoclonal antibodies: erenumab, fremanezumab, galcanezumab, the most targeted preventive option with the fewest systemic side effects
Finding the right preventive medication often takes some trial, and that process can be frustrating. Please don't give up on prevention if the first option doesn't work well. Different medications suit different people.
Tracking and Pattern Recognition
Because migraine without aura lacks the obvious warning of visual aura, keeping a detailed attack diary is especially important. Tracking:
- Date, time, duration, and severity of each attack
- Associated symptoms (nausea, light and sound sensitivity)
- Potential triggers in the 24 hours before the attack
- Medications taken and their effect
...allows you and your neurologist to identify patterns that are invisible in real-time memory: hormonal timing, weather correlations, sleep relationships. This information is not just clinically useful. It can also help you feel less at the mercy of a condition that can otherwise seem completely random.
Use Migraine Trail to automatically correlate your attack history with weather data, log attacks by voice in seconds, and generate structured PDF reports for your neurologist appointments.