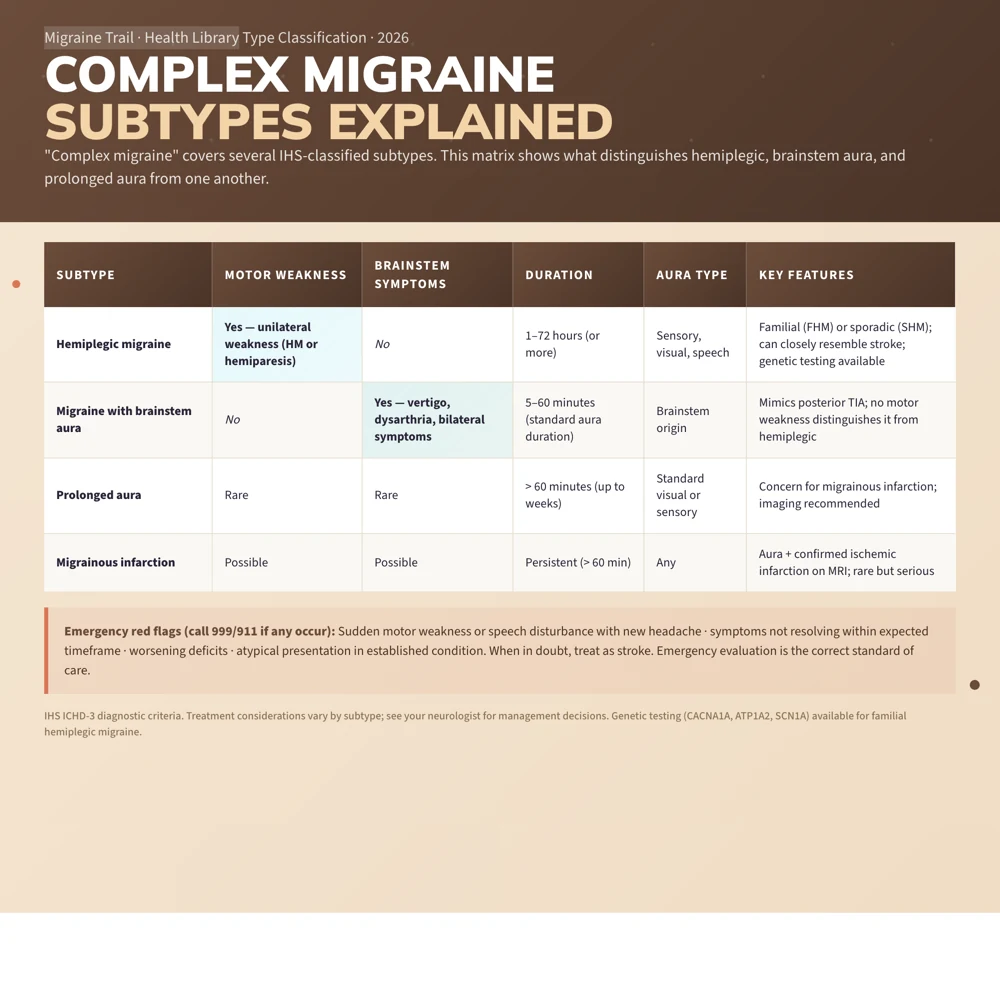
"Complex migraine" or "complicated migraine" is an informal term for migraine attacks that include neurological symptoms beyond typical visual aura, such as motor weakness, speech disturbance, unilateral sensory loss, or prolonged deficits. The term covers several distinct IHS-classified subtypes including hemiplegic migraine, migraine with brainstem aura (previously called basilar migraine), and prolonged aura. These subtypes are often confused with TIA or stroke, require careful evaluation, and may need specialist management.
Being told you have "complex migraine" can feel like both a relief and a burden. A relief because it finally explains the frightening episodes you have been having. A burden because it sounds serious, and because many people in your life may not understand why a migraine would cause weakness or affect your speech. Both reactions are valid.
The term "complex migraine" is not a formal IHS diagnosis. It is used in clinical practice and patient communities to describe migraine attacks that are more neurologically involved than standard migraine with visual aura. Understanding what falls under this umbrella, and what doesn't, matters because treatment choices, particularly around triptans and contraception, differ significantly.
What "Complex Migraine" Actually Means
Neurologists who use the term "complex" or "complicated" migraine typically mean one of the following IHS-classified conditions:
1. Hemiplegic Migraine
The most commonly meant diagnosis when "complex migraine" is used.
Hemiplegic migraine involves fully reversible motor weakness affecting one side of the body as part of the aura. The weakness (hemiplegia or hemiparesis) may last from 1 hour to several days, and in some cases persists for weeks. It is almost always accompanied by sensory aura, visual aura, or speech disturbance.
Two forms exist:
- Familial hemiplegic migraine (FHM): Autosomal dominant; caused by mutations in CACNA1A, ATP1A2, or SCN1A genes. At least one first- or second-degree relative has the same type of attack.
- Sporadic hemiplegic migraine (SHM): Same clinical picture but no family history. Same diagnostic criteria.
Because hemiplegic migraine closely resembles stroke, emergency evaluation is standard for any first or atypical presentation. See the dedicated hemiplegic migraine guide for full detail.
2. Migraine with Brainstem Aura (Basilar Migraine)
Formerly called "basilar artery migraine" or "basilar migraine," this subtype involves aura symptoms originating from the brainstem:
- Dysarthria: slurred or difficult speech
- Vertigo: true rotational vertigo (overlap with vestibular migraine is recognized)
- Tinnitus
- Hypacusis: reduced hearing
- Diplopia: double vision
- Ataxia: unsteady gait, incoordination
- Decreased level of consciousness
- Bilateral sensory symptoms simultaneously (not just one side)
Importantly, motor weakness is absent in migraine with brainstem aura. If motor weakness is present, the correct diagnosis is hemiplegic migraine.
The brainstem symptoms, which mimic posterior circulation TIA, make this subtype clinically alarming. The headache typically follows (commonly at the back of the head) or accompanies the aura symptoms.
3. Migraine with Prolonged Aura
Standard aura lasts 5 to 60 minutes. Aura lasting more than 60 minutes is atypical. Aura lasting more than 1 week without infarction is classified as persistent aura without infarction.
Prolonged aura is concerning because it may represent:
- Simply the tail end of a longer-than-usual aura (the most common explanation)
- Migrainous infarction: actual ischemia occurring during a typical aura attack
- A different diagnosis entirely
Any aura lasting more than 60 minutes warrants neurological evaluation, particularly on first presentation.
4. Migrainous Infarction
A rare but serious complication where one or more aura symptoms persist beyond 60 minutes and neuroimaging shows ischemic infarction in the relevant territory. This is the mechanism behind the elevated stroke risk in migraine with aura. It is uncommon, but it is the reason that persistent or unusual aura always needs assessment.
How Complex Migraine Differs from Standard Migraine With Aura
The difference is one of degree and type of neurological involvement:
| Feature | Typical Migraine With Aura | Complex / Hemiplegic / Brainstem | |---|---|---| | Visual symptoms | Zigzag lines, scotoma | May be present | | Sensory symptoms | Tingling (unilateral, spreading) | May be more severe or bilateral | | Motor weakness | Absent | Present (hemiplegic) | | Speech disturbance | Rare | Common in hemiplegic and brainstem | | Brainstem symptoms | Absent | Prominent in brainstem aura | | Duration | 5 to 60 minutes | Can last hours to days | | Reversibility | Fully reversible | Usually fully reversible | | TIA confusion | Low risk | High risk |
Red Flags: When to Call Emergency Services
Hemiplegic migraine and migraine with brainstem aura can be indistinguishable from stroke or TIA on clinical grounds alone, particularly during a first episode. Please call emergency services (999 or 911) if:
- Sudden severe headache with motor weakness or speech disturbance (any first episode)
- Symptoms are not resolving within the expected timeframe
- You have no prior history of this type of attack
- Neurological deficits are worsening rather than following the usual spreading aura pattern
- There are cardiovascular risk factors (hypertension, diabetes, atrial fibrillation)
Even in people with an established hemiplegic migraine diagnosis, an atypical attack warrants evaluation. The guiding principle is: when in doubt, treat as stroke. This is not overcaution. It is the correct standard of care.
Diagnosis
Diagnosis of complex migraine subtypes requires:
- Detailed history: multiple episodes with a consistent pattern, family history (for FHM), and careful description of symptom sequence and timing
- Neuroimaging: MRI brain (ideally with DWI sequence to exclude acute infarction) during or after a severe or first atypical episode
- Neurological examination: between attacks is usually normal; examination during an attack may show genuine focal deficits
- Exclusion of alternative diagnoses: stroke, TIA, CADASIL, epilepsy, MS, AVM
Genetic testing for CACNA1A, ATP1A2, or SCN1A mutations may be offered when familial hemiplegic migraine is suspected.
Getting a diagnosis can take time and require persistence. You may need to be seen by a specialist. That process is difficult, especially when episodes are frightening and recurring, but a clear diagnosis genuinely changes what treatment options are available to you.
Treatment Considerations
Acute Treatment
Triptans are generally avoided in hemiplegic migraine and migraine with brainstem aura. This is the standard guideline recommendation, though evidence that they cause harm is limited. The theoretical concern is vasoconstriction in already compromised vessels. Most specialists use NSAIDs and antiemetics as first-line:
- Naproxen sodium 500 to 1000mg early in the attack
- Prochlorperazine or metoclopramide for nausea
- Ketorolac IM for severe attacks not responding to oral medications
For brainstem aura attacks without motor features, some neurologists do use triptans pragmatically; this is an individualized decision made with your specialist.
Gepants (ubrogepant, rimegepant) work via CGRP receptor antagonism rather than vasoconstriction, and do not carry the same theoretical concerns. They are increasingly used in complex migraine subtypes where triptans are avoided.
Preventive Treatment
Preventive therapy is recommended for all people with hemiplegic migraine. Evidence-based options include:
- Verapamil or flunarizine: calcium channel blockers are often preferred first-line given their theoretical safety profile in this context
- Valproate: good evidence; avoid in women of childbearing age without contraception (teratogenic)
- Lamotrigine: particularly for brainstem aura subtype
- Acetazolamide: specifically for FHM with CACNA1A mutations (channelopathy mechanism)
- CGRP monoclonal antibodies: increasing use; accumulating case series data suggests meaningful benefit
Contraception
Migraine with any aura, including complex subtypes, combined with estrogen-containing contraceptives significantly increases stroke risk. Combined oral contraceptives are contraindicated in migraine with aura. Progesterone-only methods are safe and effective. Please discuss this explicitly with your doctor if you are currently taking or considering combined hormonal contraception.
Tracking Complex Migraine
Because complex migraine attacks are often alarming and can have real-world legal implications (such as driving restrictions in some countries), keeping a precise record of each attack is genuinely important:
- Exact sequence of aura symptoms and their duration
- Any motor, speech, or consciousness involvement
- Time to full resolution
- Medications taken and their response
This record helps neurologists distinguish stable, established hemiplegic migraine from evolving presentations that need re-evaluation, and provides documentation for driving licence decisions, workplace accommodations, and ongoing care decisions.
Use Migraine Trail to log attack details by voice, track the sequence of aura symptoms, and generate structured PDF reports for neurology appointments. The temporal pattern captured in that data is essential for managing complex migraine well, and for making sure your care team has the full picture of what you are living with.