Stress migraines and anxiety migraines share a final common pathway — both raise muscle tension and shift brain chemistry in ways that trigger migraine pain — but the root cause is different. Stress migraines are triggered by external pressure (work, deadlines, life events) and often feel tight and band-like, with pain peaking during or just after the stressful event. Anxiety migraines are driven by internal worry, overthinking, and persistent low-level dread; they tend to throb, build gradually without a specific trigger, and bring strong sensitivity to light and sound. Identifying which pattern fits your attacks changes what actually helps relieve them.
If your migraines flare every time a project deadline hits, that is a different problem than migraines that ramp up the night before a deadline you have already finished. Both are valid. Both are treatable. But the levers you pull are not the same — and the wrong intervention on the wrong type can leave you frustrated and still in pain. This guide separates the two so you can target what is actually driving your attacks.
What is a stress migraine?
A stress migraine is a migraine attack triggered by acute or chronic external pressure: work demands, family responsibilities, financial worry, sleep loss, illness, or a major life event. The brain's stress response — elevated cortisol, increased muscle tension in the neck and shoulders, vasoconstriction followed by vasodilation — directly lowers the threshold for a migraine attack in susceptible people.
A few hallmark features:
- Trigger is identifiable. You can usually point to "this week was brutal" or "we just moved house" as the cause.
- Pain is often tight and band-like, with pressure around the forehead, temples, or base of the skull.
- Onset is during or just after the stressful event. The "weekend migraine" — where the attack hits Saturday morning after a stressful workweek — is a classic stress migraine pattern, caused by the sudden drop in cortisol.
- Neck and shoulder tension is prominent, and many people feel exhausted before the pain even peaks.
- Duration is usually a few hours to a couple of days, easing as the stressor passes.
Stress is the single most commonly reported migraine trigger across surveys of people with migraine — roughly 70 to 80% identify it as a major contributor. For more on how stress sets off attacks at the physiological level, see stress and headaches connection.
What is an anxiety migraine?
An anxiety migraine is a migraine triggered by sustained internal worry, fear of the future, or persistent low-level dread — even when there is no acute external stressor. People with generalized anxiety, panic disorder, or chronic worry patterns experience migraine at roughly twice the rate of the general population, and the attacks tend to look and feel different from stress migraines.
Distinguishing features:
- Trigger is often invisible. There may be no specific event you can point to. The migraine arrives because anxiety has been steadily elevated for days or weeks.
- Pain is often throbbing or sharp, more clearly migraine-like (versus the band-like quality of a stress migraine).
- Sensitivity to light and sound is pronounced, often early in the attack.
- Nausea and restlessness frequently accompany the pain — anxiety amplifies the autonomic symptoms of migraine.
- Difficulty concentrating, racing thoughts, and a sense of "wired but tired" are common alongside the head pain.
- Duration is more variable — attacks can last longer than stress migraines and may come and go in waves over several days.
If anxiety is a regular companion to your migraines, anxiety and chronic headaches goes deeper on the bidirectional loop and what to do about it.
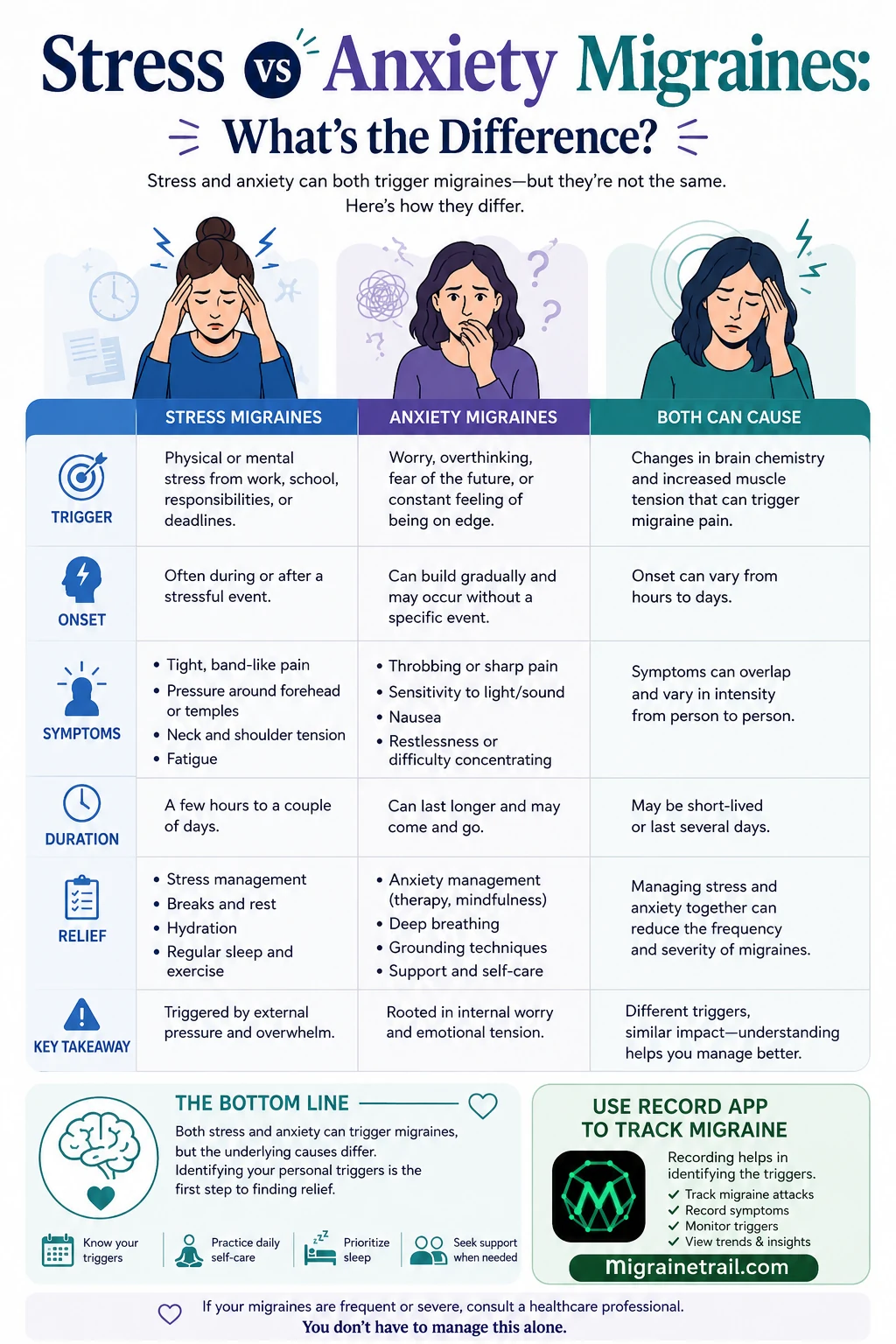
Side-by-side: stress migraine vs anxiety migraine
| Feature | Stress Migraine | Anxiety Migraine | |---|---|---| | Trigger | External: work, deadlines, life events | Internal: worry, overthinking, dread | | Onset | During or just after a stressful event | Builds gradually, often without a specific event | | Pain quality | Tight, band-like, pressure around forehead/temples | Throbbing, sharp, more classically migraine-like | | Associated symptoms | Neck and shoulder tension, fatigue | Light/sound sensitivity, nausea, restlessness | | Duration | A few hours to a couple of days | Variable; can last longer and recur in waves | | What helps most | Stress management, breaks, sleep, exercise | Therapy (CBT), mindfulness, grounding, deep breathing | | What does NOT help much | Reassurance alone — needs load reduction | Pushing through — needs to address the worry pattern |
Both can also occur in the same person, sometimes within the same week. Stress and anxiety often co-trigger each other: a stressful event causes worry, the worry persists after the event ends, and the migraine pattern shifts from acute (stress) to sustained (anxiety).
How to tell which is driving yours
Most people guess wrong on first reflection. The most reliable way to know is to track several attacks and look for patterns:
- For each attack, log what was happening in the 24 to 48 hours before. Was there a specific event you can name? Or a vague "I have been worried all week" feeling?
- Note the pain quality at onset. Tight and pressing → leans stress. Throbbing with early light sensitivity → leans anxiety.
- Notice what you were doing when it started. Mid-deadline → stress. Lying in bed at night thinking about tomorrow → anxiety.
- Pay attention to what helps. A nap and a hot shower easing the pain → stress. Needing to actively quiet your thoughts before the pain eases → anxiety.
Over 30 to 60 days of consistent logging, most people see a dominant pattern. Some discover they have both, on different days. The identifying hidden migraine patterns guide walks through the analysis approach.
Why the distinction matters for treatment
The acute medication (triptan, gepant, NSAID) is the same regardless of trigger — see how to stop a migraine fast for the acute playbook. Where stress and anxiety migraines diverge is in prevention:
For stress-driven migraines, what reduces frequency most:
- Workload management and protected recovery time after high-demand periods (heading off the weekend migraine).
- Regular sleep schedule and consistent meal timing.
- Aerobic exercise 3 to 5 times per week — meta-analyses show ~30% reduction in attack frequency.
- Magnesium supplementation (400mg/day, with clinician sign-off).
- Beta-blockers (propranolol) are often a strong preventive choice because they blunt the physiological stress response itself.
For anxiety-driven migraines, what reduces frequency most:
- Cognitive behavioral therapy (CBT) — strong evidence for reducing both anxiety and migraine frequency.
- Mindfulness-based stress reduction (MBSR) — 8-week programs cut migraine days by ~30% in trials.
- SSRIs or SNRIs, prescribed for the underlying anxiety, often also reduce migraine frequency.
- Tricyclic antidepressants (amitriptyline at low dose) — dual action on anxiety and migraine prevention.
- Limiting caffeine — caffeine amplifies anxious physiology and is a sneaky contributor to anxiety-driven attacks.
Treating an anxiety-pattern migraine with workload management alone will underperform. Treating a stress-pattern migraine with mindfulness alone will too. Matching the intervention to the driver is the entire point of figuring out which is yours.
When both are present
Many people with chronic migraine have both stress sensitivity and an anxiety pattern operating at once. If that fits you:
- Address the anxiety first. Anxiety amplifies stress reactivity, so reducing the baseline anxiety often shrinks stress migraine frequency as well.
- CBT and SSRIs are first-line for the anxiety component; preventive migraine medication (CGRP monoclonal antibody, beta-blocker, or tricyclic) can be layered on for the migraine component.
- Track both stressful events AND your subjective anxiety level (a 1 to 10 daily check-in) — the two will diverge in ways that reveal the dominant driver of any given week.
Comorbid depression is also common with anxiety and migraine — see migraine depression connection for the related pattern.
Frequently asked questions
Can stress alone cause a migraine?
In someone genetically predisposed to migraine, yes. Stress lowers the migraine threshold by raising cortisol, increasing muscle tension, and shifting serotonin signaling — all of which can trigger an attack in a susceptible brain. Stress does not "give" people migraine; it triggers attacks in people whose nervous system is already migraine-prone.
Can anxiety cause migraines or are they just headaches?
Both. Anxiety can trigger a true migraine (with throbbing, light sensitivity, nausea, sometimes aura) and it can also cause tension-type headache (tight, band-like, no nausea). The two often coexist. The presence of nausea, light/sound sensitivity, or aura points to migraine rather than tension headache.
Why do I get migraines on weekends?
The classic "weekend migraine" is a stress migraine. During the workweek, elevated cortisol suppresses the attack. When you finally relax on Saturday morning, cortisol drops sharply and the migraine that was being held back arrives. Going to bed and waking up at the same time on weekends — and not sleeping in too late — substantially reduces weekend migraine frequency.
What is the fastest way to stop a stress or anxiety migraine?
Treat early with acute medication, get to a dark and quiet space, hydrate, and use a cold compress on the head or neck. For the underlying trigger, brief grounding exercises (4-7-8 breathing, the 5-4-3-2-1 sensory check) help anxiety-driven attacks; a hot shower or 20-minute nap helps stress-driven attacks. Full acute treatment playbook: how to stop a migraine fast.
Should I see a doctor if my migraines are stress or anxiety related?
Yes, especially if you have more than 4 attacks per month, your acute medication is not working, you are using acute medication more than 10 days per month, or anxiety is affecting daily function. Migraine + anxiety responds well to combined treatment, but it needs a clinician to coordinate. Bring 30+ days of attack tracking data to the appointment — it dramatically improves the conversation.
What this means for you
Stress and anxiety migraines look similar on the outside but respond to different interventions. The fastest way to figure out which pattern is yours is to track attacks alongside what was happening before them — stressful events, worry levels, sleep, caffeine, exercise — for 30 to 60 days. Patterns become visible within weeks once the data exists.
Track in seconds with Migraine Trail's free voice logging — capture the attack, the trigger context, and how it resolved without typing. Bring the resulting timeline to your clinician and the path forward usually becomes obvious.
Sources
- American Migraine Foundation. Migraine and anxiety.
- Buse DC, et al. Psychiatric comorbidities of episodic and chronic migraine. Journal of Neurology.
- Minen MT, et al. Migraine and its psychiatric comorbidities. Journal of Neurology, Neurosurgery & Psychiatry.
- Lipton RB, et al. The role of stress in the etiology of migraine. Headache.
- International Classification of Headache Disorders, 3rd ed. (ICHD-3).
- National Institute of Mental Health (NIMH). Anxiety disorders.